
Introducing a new tool we have added to our clinic, filling a gap in the screening for early cognitive deficits … dementia. For an overview of the full screening process, please see our blog titled Neurocognitive Screening.

It is challenging to make a diagnosis of dementia in the earliest stages. For some forms, there are specific findings that can lead toward early diagnosis, and some of these are visual findings.
Whereas there are a few diagnostic markers available once a problem has been identified, such as p-tau 217, Beta amyloid, ApoE gene markers, and MRI, they are basically “late to the game”. It’s EARLY SCREENING that is needed. Typical screening involves a paper based test that misses a significant component … visuospatial, and how that is integrated into what we call executive function. It is known that visuospatial tracking and visual memory correlate fairly well with early disease onset before some of the other things become apparent. It is the visuospatial screening that has been difficult to do in a primary care setting, but finally there are ways to get that done … one of those is via the machine called Cognivue.
(The next few paragraphs get a bit technical. It’s always hard to know who wants to know how much detail. But, forewarned …)
The machine tests what we call visuospatial function. Broadly defined, visuospatial function is the ability to specify the parts and overall configuration of a percept (a mental concept that is developed as a consequence of the process of perception), appreciate its position in space, integrate a coherent spatial framework, and perform mental operations on spatial concepts. Visuospatial function is commonly conceptualized in three components: visual perception, visual construction, and visual memory.
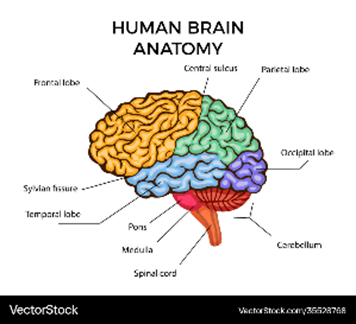
• Visual perception involves light perception, contrast sensitivity, stimulus orientation, visual acuity, detection of color and motion, and processes mediated primarily by the occipital cortices.
• Visual construction involves multiple areas of the brain putting things together (the parietal, temporal, and frontal cortices).
• Visual memory consists of two main components: recall of visual information and topographical memory.
Visuospatial dysfunction is among the earliest manifestations in some dementias, eventually affecting >20% of those patients. One study showed disabling visuospatial disorientation in more than one-third of dementia patients, while almost half of patients complained of visuospatial problems when questioned directly. Patients may describe impaired discrimination of form, colors and contrast, motion detection, as well as disturbances of higher order functions such as reading, visuospatial orientation, and visual search strategies.
You can see how complicated the entire process is, and traditional testing does not engage this aspect. That is why we are so pleased to have an additional tool. Now that we have reviewed the what and the why, let’s discuss the machine itself.

It’s called Cognivue and it is in our office. The device is a self-administered, digital cognitive assessment that standardizes the patient’s experience and removes the bias that can exist with traditional testing methods. The technology collects over 130,000 data points and is highly sensitive to each individual patient. It uses something called adaptive psychophysics, creating a unique patient experience customized to each patient’s individual visual and motor skills. It has been validated against other recognized gold-standard cognitive assessment tools, while providing an experience customized to each patient. The custom experience is important to what we do at Alliance, and the self-administered computerized process fits seamlessly into the clinic workflow. You may note that rather than using a keyboard, the entire test is done via what they call a CogniWheel. It is a simple, intuitive, and easy-to-maneuver wheel.
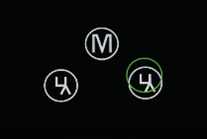
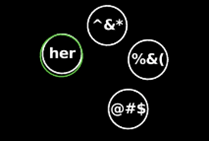
The test process itself takes the patient through a series of exercises to assess the domains of Visiospatial: Memory, Executive Function/Attention, and Discrimination, as well as two speed performance parameters. The computer screen with which the patient interacts will look a lot like the following (notice how the activity presented changes depending on the specific aspect being tested):
Motor Skills

Visual Acuity

Letter Perception
Word Perception
Shape Perception
Motion Perception
Word Memory

Letter Memory
Shape Memory
Motion Memory
The Cogniwheel is the control that allows the user to maneuver a highlighted area to select the response they wish to enter. The results are calculated via the computer, taking into account the patient error rates, reproducibility of the errors, and reaction time. Those results are compared with a large data set, placing the patient on a curve of what would be considered normal or outside of the normal range, and generates a score for each section. This is helpful because should a narrow problem be identified, it can be followed by additional investigations and potential referrals to neurology or ophthalmology. Should the test be considered “normal”, then the score is helpful as a marker for repeat screening at a later date (perhaps annually). A decline would also lead to additional investigations and potential referrals. This is an example of the report that is generated.
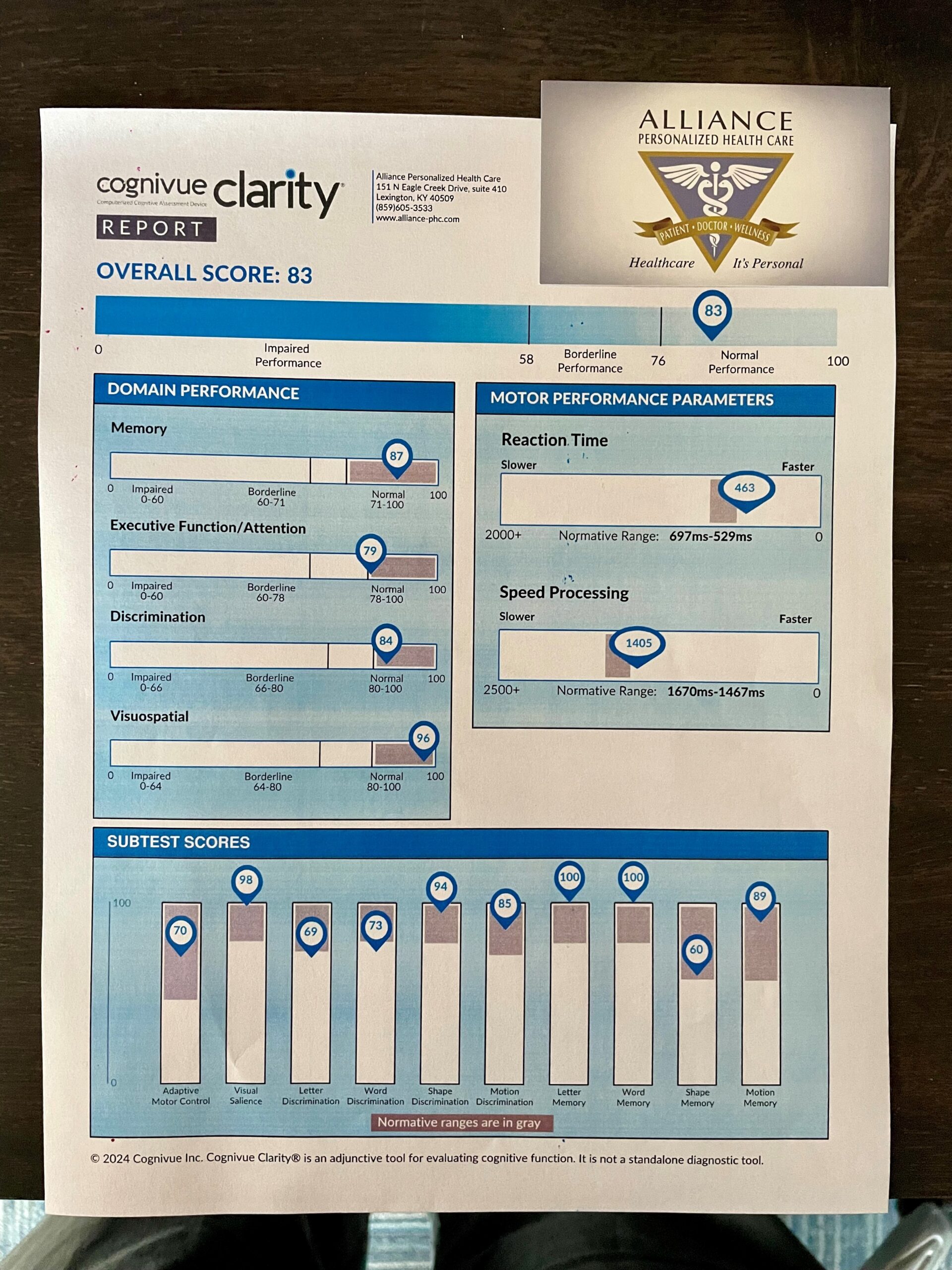
We then incorporate this information with the remainder of the cognitive screening visit, and merge all of that with what we know about you.
That concludes the overview of one more tool we have available at Alliance. This is perhaps a perfect example of integrating modern technology with your story and our experience … something we continually strive to deliver.